



In an unprecedented collaboration, a group of physicians from Massachusetts General Hospital (MGH) and Brigham and Women’s Hospital in Boston is working with about 100 architects and engineers from across the United States to develop a patient isolation hood (PIH) intended to contain the coronavirus in clinical settings and help protect health-care providers.
Led by Dr. Samuel Smith, an anesthesiologist at MGH and instructor at Harvard Medical School, architect Eric Höweler, co-partner of the Boston-based Höweler + Yoon, and faculty at Harvard’s Graduate School of Design (GSD), the development of the PIH emerged after the two hospitals created a Center for COVID Innovation, which is mobilizing experts across disciplines to research vaccines for the virus and brainstorm ways to manufacture protective equipment.

Höweler, a co-director of the effort along with Nathan Phipps, an industrial designer and researcher from Harvard’s Wyss Institute for Biologically Inspired Engineering, delivered several PIH prototypes to MGH on April 13; by Friday, April 17, they expect to have between 20 and 30 ready for a “test run” in the intensive care unit and elsewhere in the hospital. The hoods are arriving in advance of the anticipated peak of the virus surge in Massachusetts, expected to occur by the end of April. As of Monday, state public health officials confirmed 26,867 cases of COVID-19 and 844 deaths. Smith says there are currently 300 patients with the virus at MGH.
“The project brief and requirements aren’t that different from any architectural project, regardless of scale,” says Zach Seibold, a Boston architect and member of the team who specializes in emerging materials and fabrication techniques at Harvard. “We’re able to use the same fabrication tools for the hood prototypes as we do for conceptual prototypes at the GSD. The workflow and knowledge of how to interact with these machines is remarkably similar.”
Harnessing ideas from architects located in Ohio, California, New Mexico, and beyond, Höweler worked with Seibold, Phipps, Chris Hansen (a digital fabrication specialist at the GSD’s Fabrication Laboratory), Saurabh Mhatre (a research associate in the Material Processes and Systems Group at the GSD), and other faculty to deliver two types of hoods.
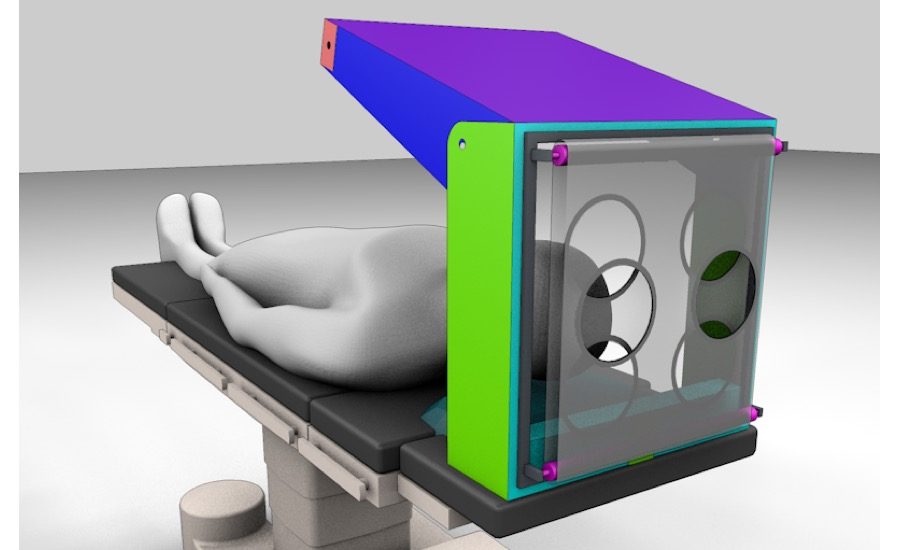
One is made from a single sheet of plastic film cut on a Zund CNC machine and folded like origami into a hood form; the other uses an adjustable rigid frame that cantilevers over the patient’s face and is fitted with transparent plastic. Both are lightweight, intuitive for doctors to operate, able to fit over any size bed or mattress, and easily removable if a doctor has to access a patient in an emergency. Aside from the reusable frame on the cantilevered prototype, the hoods are single-use to address infection control issues.

Both versions function similarly: they cover a patient’s head and torso while doctors insert a breathing tube into their mouth and airway and then attach a respirator to deliver oxygen—a common procedure for COVID-19 patients, many of whom are coughing and struggling to breathe. The hood has two holes for doctors to insert their arms and access the patient, as well as an opening for the breathing tube. Negative pressure is created inside the hood by sucking out—and away from the doctor—any aerosolized particles that might contain the virus, then pulling fresh oxygen in. A drape closes the gap between the hood and the rest of the patient’s body and is tucked under them.
The hoods were perfected over the course of the last two weeks, as the far-flung designers traded ideas back and forth, pro bono, over a fast-moving Slack channel called “Full Body Protection MGB. “It was truly a grassroots effort,” says Höweler. The architect acted as de facto manager of the process and design critic, working with local fabricator Polyfab, which is donating its time and supplies. “We’ll eventually emerge from this pandemic and hope that this has utility afterwards as well,” says Seibold.
While some design teams have been making transparent, rigid plastic boxes for doctors to use while intubating coronavirus patients, Smith and the designers say these are deeply flawed; he has even turned away deliveries to MGH. According to the doctor, they are restrictive for care providers and weigh about 25 pounds, making them hazardously heavy in emergency situations. Other do-it-yourself versions, like those made of PVC pipe frames and semi-transparent plastic film, are clunky and don’t fit all beds. “If it doesn’t function well, both ergonomically and practically, it’s not going to be useful to physicians,” he says. Smith also plans to study whether the PIH can help prevent the need for respirators—which are in short supply—simply by covering the patient and providing a high-flow nasal cannula and a lot of oxygen.
The PIH design is open source. “We want people to be able to produce this as fast as possible. You don’t worry about intellectual property at this point,” says Dr. Smith. He adds that the development of the hood would never have happened without a true collaboration between architects and medical professionals, and that the result is a product that should make the clinical environment safer for all, and therefore reduces stress. “It would have taken six months on a consulting basis, and then it probably wouldn’t have been right,” he says. “Architects need to be more involved with health care innovation and my colleagues need to understand that design matters.”




